Inhaled Management of Asthma
Find the latest updates on inhaled medications for the treatment of asthma (including their place in the 2020 updated Global Initiative for Asthma [GINA] strategy), targets for treatment and the importance of inhaler devices in drug delivery.
Unmet need in inhaled asthma care
Patients still suffer from symptoms of asthma despite the availability of effective treatments. Explore the unmet needs in asthma.
Over one-third of patients with asthma are uncontrolled on long‑acting β2‑agonist (LABA)/inhaled corticosteroid (ICS) therapy,1,2 placing them at risk of exacerbations and hospitalisation and negatively impacting their quality of life.3–5 However, studies suggest that many patients perceive their asthma to be well controlled, despite experiencing regular symptoms.5,6
The main causes of uncontrolled asthma are poor adherence and incorrect inhaler technique.4
Many (30–70%) patients do not adhere to treatment.7 A survey among patients with asthma found that patient adherence to controller therapy was generally poor, despite many patients having relatively severe and uncontrolled asthma. In addition, nonadherence to controller therapy was more prevalent among patients experiencing symptoms requiring reliever medication (two or more puffs in the previous week) compared with those requiring little or no reliever medication.8 In another survey, a large number of patients believed that they could stop using their controller therapy when their symptoms were infrequent and two-thirds of patients believed that reliever therapy could be used every day.6
Incorrect inhaler technique is a common cause of uncontrolled asthma and this is the case with both metred-dose inhalers (MDIs) and dry powder inhalers (DPIs). Even with training, half of all patients with asthma are unable to use their inhalers properly.9 With MDIs, the biggest problem is that patients do not actuate and inhale the medication at the right times; with DPIs, patients do not inhale the powder fast enough or with enough force to get the correct dose of medication to the lungs.3
If we are to address issues such as poor adherence and inhaler technique we need new strategies. In recent years, there has been an increase in the number of people using technology to monitor and manage their health and most are willing to share this information with their doctor.10 With the global digital revolution, exciting new innovations are emerging under the ‘electronic health (eHealth)’ umbrella.
Innovations may fall within categories including mobile health applications (mHealth apps) (clinical interventions supported by mobile devices) and telemedicine, which often uses telephone or electronic technology to facilitate long-distance healthcare or education.11 These technologies are designed to support the patient and their healthcare provider, improving quality of care, disease management and patient outcomes.7,11,12
For example, inhaler monitoring devices are sensors (such as the Propeller® Health Sensor) which can attach to both reliever and controller inhalers. Connected to an app, sensors track symptoms and adherence by recording when and where the inhaler was used. Reminders can even be sent to the patient or their family members when a routine treatment is missed.7,13 Promisingly, a recent study found that patients with asthma using the Propeller® Health Sensor with a short‑acting β2‑agonist (SABA) inhaler had reduced SABA use, more treatment-free days and improved asthma control test scores compared with patients who received conventional (face-to-face) care.13
The main causes of uncontrolled asthma are poor adherence and incorrect inhaler technique. Therefore, digital innovations which support patients and healthcare professionals in addressing these causes may be the future of asthma care and key to improving asthma control and outcomes for patients.
of interest
are looking at
saved
next event
Infographic – Digital and drug delivery innovations to improve adherence in asthma
Download and print this infographic to learn more about the reasons for poor adherence in patients with asthma and the drug delivery and digital innovations that can be used to address and improve poor adherence.
Content produced in May 2020.
Improving inhaled asthma care: control of inflammation and bronchodilation
Asthma is a chronic inflammatory disorder of the airways involving many different types of cells and cellular elements. In this section you can learn about how inhaled corticosteroids target inflammation in asthma and bronchodilators address bronchoconstriction. In combination, inhaled therapies have the potential to deliver control of inflammation and comprehensive bronchodilation in order to optimise outcomes in patients with asthma.
Asthma is a heterogeneous disease, often driven by chronic airway inflammation (Figure 1) and characterised by airway smooth muscle (ASM) contraction which is responsible for bronchoconstriction. This causes symptoms such as wheezing and breathlessness.1,2 The worsening of these symptoms results in asthma exacerbations.3
Anti-inflammatory therapy with inhaled corticosteroids (ICS) is the backbone of asthma treatment and is recommended for use by people with all disease severities. ICS increase transcription and expression of anti-inflammatory proteins, and repress cytokines involved in the inflammatory response (e.g. IL-4, IL-5 and chemokines involved in eosinophil recruitment).4 In this way, ICS work to effectively control airway inflammation and hyperresponsiveness, resulting in improved asthma symptoms and lung function, and a reduced frequency of exacerbations.4
Drug delivery systems for ICS should optimise on-target delivery to the lungs, depositing particles at the right site of action. An ideal ICS should have high affinity and associate rapidly with the glucocorticoid receptors, in order to exert its anti-inflammatory effect rapidly.5
In asthma, contraction of ASM is modulated by the binding of two neurotransmitters to their receptors in the lungs. Acetylcholine binds to muscarinic M3 receptors, which simultaneously causes mucus secretion, and adrenaline targets the β2-adrenoreceptors.6 It is likely that there is crosstalk between these receptors, which amplifies the bronchoconstrictive effect.6 Untreated, bronchoconstriction can result in airway remodelling (in which the airway walls thicken) and an increase in mucus secretion.6,7 Airway remodelling can lead to exacerbations and impact patients’ quality of life.3
Inhaled bronchodilators, such as long-acting β2-agonists (LABA) and long-acting muscarinic antagonists (LAMA), target bronchoconstriction and relieve asthma symptoms by relaxing ASM and clearing mucus. LABA relax ASM by stimulating β2-adrenoreceptors and LAMA primarily target M3 receptors to prevent bronchoconstriction.6 Combinations of LABA and LAMA have been found to have an additive bronchodilatory effect on the airways, which may even be enhanced by the crosstalk between the two receptors.6,8,9
The 2020 Global Initiative for Asthma (GINA) strategy recommends that patients with asthma initiate low-dose ICS with a β2-agonist as needed from Step 1. From Step 3, daily maintenance treatment with LABA/ICS is recommended, with the addition of a LAMA from Step 4, to effectively treat asthma symptoms and reduce asthma exacerbations.1,2,6
Most patients can be treated effectively with low doses of ICS, but medium doses may be needed if patients still have uncontrolled asthma despite good adherence and inhaler technique.1 For the few patients requiring high-dose ICS, the risk:benefit profile should be carefully considered. It is important to monitor the response to treatment and any side effects and to adjust the dose accordingly.1
Delivering anti-inflammatory effects and comprehensive bronchodilation through LABA/LAMA/ICS combination therapy has the potential to successfully reduce airway inflammation, improve the symptoms of asthma and ultimately reduce exacerbations and airway remodelling.
Recent and ongoing trials are investigating the use of LABA/LAMA/ICS combination therapies for asthma, holding promise that LABA/LAMA/ICS may be the future standard of treatment for patients with moderate‑to‑severe asthma currently treated with medium-to‑high doses of LABA/ICS.
Figure 1. Persistent inflammation in the airway may lead to structural changes, such as mucus hypersecretion, smooth muscle hyperplasia, subepithelial fibrosis, blood vessel proliferation, and infiltration of inflammatory cells.

Figure 2. Asthmatic airways are characterised by thickened and inflamed walls, which, alongside airway smooth muscle contraction and mucus hypersecretion, can lead to exacerbations.
of interest
are looking at
saved
next event
Improving inhaled asthma care: inhaler devices
It’s critical that inhaled medication is delivered in an inhaler the patient can actually use. In this section you can read about the range of inhalers available for delivery of asthma medication and factors to consider when deciding on an inhaler for an individual patient.
Inhaled treatment is the preferred route of delivery for asthma medication as inhalers deliver drugs rapidly and directly to the airways.1 Controller inhalers contain anti‑inflammatory medication such as inhaled corticosteroid (ICS) and are used on an as-needed or daily basis, depending on the severity of asthma, whereas reliever inhalers aim to relieve symptoms quickly.1
Most patients (up to 70–80%) with asthma are unable to use their inhaler correctly and the majority are unaware of this.1 Even with training, 50% of patients with asthma are unable to use their inhalers properly.2 Furthermore, 30–70% of patients do not adhere to treatment.3 This is important because poor adherence may lead to an increased risk of severe exacerbations.3,4 Compliance to prescribed medication aims to reduce, and possibly even eliminate, the need for reliever medication.1,3
Inhalers for asthma include metred-dose inhalers (MDIs), which may be pressurised or propellant-free, and dry powder inhalers (DPIs), both of which provide fixed doses.5 MDIs require patients to coordinate their breathing to the release of the aerosol, whereas DPIs do not require this coordination as the drug is delivered in powder form.5,6
Both MDIs and DPIs are considered easy to use; however, DPIs may be slightly easier than MDIs.5 To reduce the speed of aerosol release and improve the efficiency of the aerosol delivery in MDIs, spacers or valved holding chambers can be added.7 To use DPIs, patients need to use great force to disperse the powder in the inhaler before inhalation.7 One problem with DPIs is that they can be affected by humidity and environment.7 There is inconsistent data in favour of either inhaler type.5
The CRITIKAL study assessed inhaler errors in 3,660 patients with asthma using either MDIs or DPIs. Common errors were found in patients using both inhalers: approximately a third of patients were not tilting their chin up during inhalation and between 25.4–32.4% of patients did not exhale before using the inhaler. Regarding each individual type of inhaler, actuation before inhalation occurred in 24.9% patients using MDIs and was associated with uncontrolled asthma. Additionally, 47.2% did not provide inspiratory effort that was slow and deep enough. Similarly, a number of patients (32–38%) using DPIs provided insufficiently fast or forceful inspiratory effect, which was associated with poor control and an increased rate of exacerbations.8
With every inhalation device, it is important to check patient's inhaler technique at every opportunity, to ensure they are using their inhaler correctly and effectively.1 An ideal inhaler should provide consistent and efficient drug delivery and be easy to use,6 thus avoiding critical errors. The BREEZHALER® is an example of a DPI that provides a dose of treatment in a transparent capsule, which allows the patient to see that the full dose has been taken.
The choice of inhaler for an individual patient will depend on various factors including: medication options available in the device, patient preference, patient ability to use the inhaler and cost.1
of interest
are looking at
saved
next event
GINA strategy recommendations
What is the place of inhaled medications in the treatment of asthma? Scroll down to find out about recommendations in the 2021 updated Global Initiative for Asthma (GINA) strategy!
The Global Initiative for Asthma (GINA) aims to increase awareness of asthma among health professionals, health authorities and the general public.1 Each year, the GINA Scientific Committee review state‑of‑the‑art literature and update the GINA global strategy for asthma management and prevention; the GINA 2021 reports can be found here.
Inhaled therapies underpin the GINA strategy stepwise approach to asthma management (Figure 1).1
All adults and adolescents with asthma should receive inhaled corticosteroid (ICS)‑containing controller therapy to reduce their risk of exacerbations and control symptoms.1 Patients should be encouraged to adhere to their controller medication even when symptoms are infrequent, to reduce or eliminate the need for reliever therapy.
The GINA 2021 treatment strategy for adults and adolescents recommends two “tracks”, based on the choice of reliever medication: either as-needed low-dose ICS-formoterol (‘Track 1’), or as-needed short-acting β2-agonist (SABA; ‘Track 2’).1
To find out more about the 2021 updates and clinical implications, watch the Spotlight GINA 2021 webinar here.
Figure 1. Current Global Initiative for Asthma (GINA) recommendations for the treatment of asthma.1 ©2021 Global Initiative for Asthma, available from www.ginasthma.org, reprinted with permission. HDM = house dust mite; ICS = inhaled corticosteroid; LABA = long-acting beta-agonist; LAMA: long-acting muscarinic antagonist; LTRA = leukotriene receptor antagonist; OCS = oral corticosteroids; SABA = short-acting beta-agonist; SLIT = sublingual immunotherapy.
of interest
are looking at
saved
next event
Recent clinical trials
Recommendations for inhaled therapies for patients with asthma are continually evolving, based on the latest evidence and understanding of the disease.
In this section, you can discover up-to-date information on recent and ongoing clinical trials exploring the efficacy and safety profiles of long-acting β2-agonist/long-acting muscarinic antagonist/inhaled corticosteroid (LABA/LAMA/ICS) and LABA/ICS combination therapies.
Research continues apace to provide insights into the role of inhaled combination therapies in asthma.
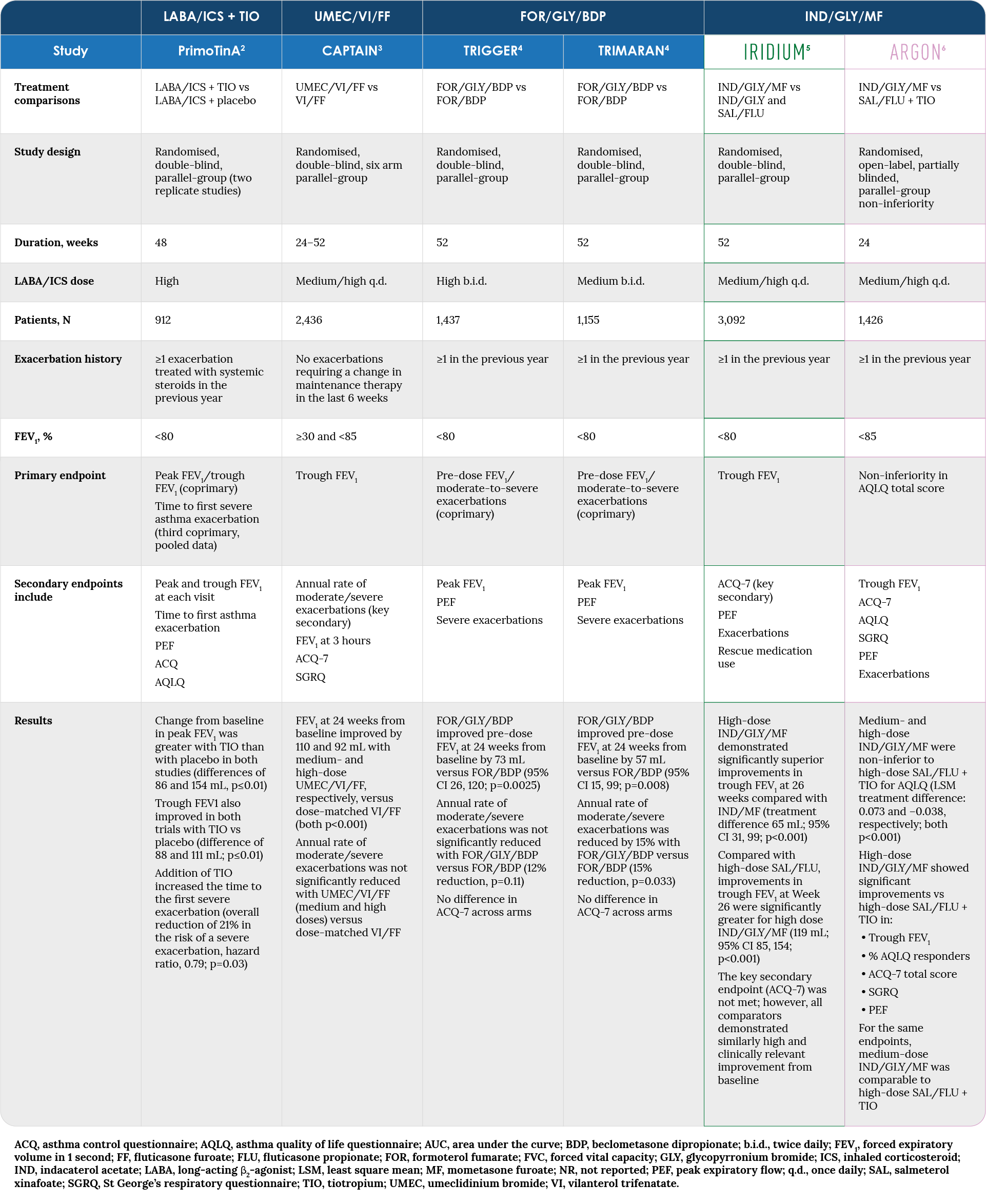
Table 1 summarises available information on the study designs and key results for recent clinical trials investigating the use of new LABA/LAMA/ICS combination therapies for the treatment of asthma.
Evidence was provided by the PrimoTinA study, in which the LAMA tiotropium was added to LABA/ICS in free combination. Subsequently, fixed LABA/LAMA/ICS inhaled combinations have been developed. These include umeclidinium bromide/vilanterol trifenatate/fluticasone furoate (UMEC/VI/FF), assessed in the CAPTAIN study, and formoterol/glycopyrronium/beclometasone dipropionate (FF/GLY/BDP), assessed in the TRIMARAN and TRIGGER studies.
IRIDIUM and ARGON, part of the Phase III clinical programme , investigated the efficacy and safety profile of inhaled combination indacaterol acetate/glycopyrronium bromide/mometasone furoate (IND/GLY/MF) in patients with uncontrolled asthma despite medium- or high-dose LABA/ICS.
The GINA 2021 report now recommends IND/GLY/MF, UMEC/VI/FF and FF/GLY/BDP as preferred treatment options for patients at Step 5, and ‘other’ options for patients at Step 41.
Table 1. LABA/LAMA/ICS and LABA/ICS + LAMA combination trials: study designs and key results
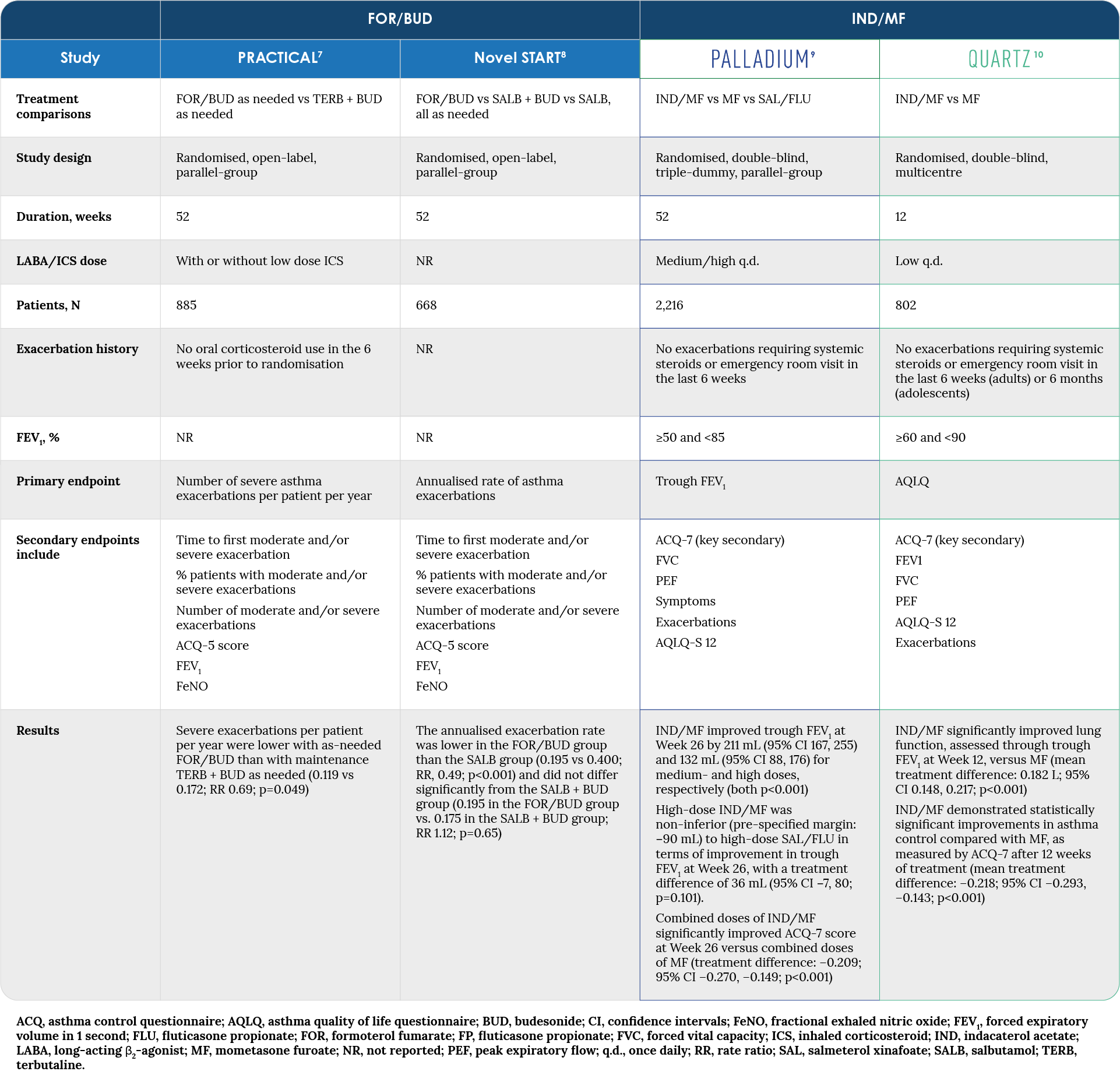
While LABA/ICS combinations are well established in clinical practice, new research is available on their role in mild asthma, as well as on novel LABA/ICS combinations. Table 2 presents an overview of the very latest trials. These include the Novel START study and the PALLADIUM and QUARTZ studies (part of the programme) which investigate the efficacy and safety profile of IND/MF in patients with uncontrolled asthma despite medium- or high-dose ICS or low-dose LABA/ICS (PALLADIUM), or low-dose ICS (QUARTZ).
Table 2. LABA/ICS combination trials reporting in 2019: study designs and key results
of interest
are looking at
saved
next event
References
Unmet need in inhaled asthma care, Improving inhaled asthma care: control of inflammation and bronchodilation, Improving inhaled asthma care: inhaler devices, GINA strategy recommendations, Recent clinical trials.
Unmet need in inhaled asthma care
- Bateman ED, Boushey HA, Bousquet J, et al. Can guideline-defined asthma control be achieved? The Gaining Optimal Asthma ControL study. Am J Respir Crit Care Med 2004;170:836–844.
- Fang J, Busse WW, Marvel J, Tian H, Altman P, Cao Hl. Demographic, clinical characteristics and control status of pediatric, adolescent and adult asthma patients by GINA Step in a US longitudinal cohort. Am J Resp Crit Care Med 2018;197:A1903 (Abstract).
- Price DB, Román-Rodríguez M, McQueen RB, et al. Inhaler errors in the CRITIKAL study: type, frequency, and association with asthma outcomes. J Allergy Clin Immunol Pract 2017;5:1071–1081.
- Global Initiative for Asthma (GINA 2020). Global strategy for asthma management and prevention. Last accessed July 2020. Available from: www.ginasthma.org.
- Katsaounou P, Odemyr M, Spranger O, et al. Still fighting for breath: a patient survey of the challenges and impact of severe asthma. ERJ Open Res 2018;4:pii:00076–2018.
- Sastre J, Fabbri LM, Price D, et al. Insights, attitudes, and perceptions about asthma and its treatment: a multinational survey of patients from Europe and Canada. World Allergy Organ J 2016;9:13.
- Asthma UK. Connected asthma: how technology will transform care. Last accessed July 2020. Available from: https://www.asthma.org.uk/f29019fc/globalassets/get-involved/external-affairs-campaigns/publications/connected-asthma/connected-asthma---aug-2016.pdf.
- Bender BG, Long A, Parasuraman B, Tran ZV. Factors influencing patient decisions about the use of asthma controller medication. Ann Allergy Asthma Immunol 2007;98:322–328.
- Azzi E, Srour P, Armour C, Rand C, Bosnic-Anticevich S. Practice makes perfect: self-reported adherence a positive marker of inhaler technique maintenance. NPJ Prim Care Respir Med 2017;27:29.
- Accenture Consulting. 2018 Consumer survey on digital health: US results. 2018. Last accessed July 2020. Available from: https://www.accenture.com/t20180306t103559z__w__/us-en/_acnmedia/pdf-71/accenture-health-2018-consumer-survey-digital-health.pdf.
- Jeminiwa R, Hohmann L, Qian J, Garza K, Hansen R, Fox BI. Impact of eHealth on medication adherence among patients with asthma: a systematic review and meta-analysis. Respir Med 2019;149:59–68.
- Matricardi MP, Dramburg S, Alvarez-Perea A, et al. The role of mobile health technologies in allergy care: An EAACI position paper. Allergy 2019:doi: 10.1111/all.13953. [Epub ahead of print].
- Merchant RK, Inamdar R, Quade RC. Effectiveness of population health management using the Propeller Health Asthma Platform: a randomized clinical trial. J Allergy Clin Immunol Pract 2016;4:455–463.
Improving inhaled asthma care: control of inflammation and bronchodilation
- Global Initiative for Asthma (GINA 2020). Global strategy for asthma management and prevention. Last accessed July 2020. Available from: www.ginasthma.org.
- Kaczmarek KA, Clifford RL, Knox AJ. Epigenetic changes in airway smooth muscle as a driver of airway inflammation and remodeling in asthma. Chest 2019;155:816–824.
- Barnes PJ, Szefler SJ, Reddel HK, Chipps BE. Symptoms and perception of airway obstruction in asthmatic patients: clinical implications for use of reliever medications. J Allergy Clin Immunol 2019;144:1180–1186.
- Barnes PJ. Efficacy of inhaled corticosteroids in asthma. J Allergy Clin Immunol 1998;102:531–538.
- Derendorf H, Nave R, Drollmann A, Cerasoli F, Wurst W. Relevance of pharmacokinetics and pharmacodynamics of inhaled corticosteroids to asthma. Eur Respir J 2006;28:1042–1050.
- Gosens R, Gross N. The mode of action of anticholinergics in asthma. Eur Respir J 2018;52:pii: 1701247.
- Fehrenbach H, Wagner C, Wegmann M. Airway remodelling in asthma: what really matters. Cell Tissue Res 2017;367:551–569.
- Blais CM, Davis BE, Cockcroft DW. The effect of glycopyrronium and indacaterol, as monotherapy and in combination, on the methacholine dose-response curve of mild asthmatics: a randomized three-way crossover study. Respir Res 2017;18:146.
- Davis BE, Blais CM, Cockcroft DW. Methacholine challenge testing: comparative pharmacology. J Asthma Allergy 2018;11:89–99.
Improving inhaled asthma care: inhaler devices
- Global Initiative for Asthma (GINA 2019). Global strategy for asthma management and prevention. Last accessed July 2020. Available from: www.ginasthma.org.
- Azzi E, Srour P, Armour C, Rand C, Bosnic-Anticevich S. Practice makes perfect: self-reported adherence a positive marker of inhaler technique maintenance. NPJ Prim Care Respir Med 2017;27:29.
- Asthma UK. Connected asthma: how technology will transform care. 2016. Last accessed July 2020. Available from: https://www.asthma.org.uk/f29019fc/globalassets/get-involved/external-affairs-campaigns/publications/connected-asthma/connected-asthma---aug-2016.pdf.
- Engelkes M, Janssens HM, de Jongste JC, Surkenboom MC, Verhamme KM. Medication adherence and the risk of severe asthma exacerbations: a systematic review. Eur Respir J 2015;45:396–407.
- Ramadan WH, Sarkis AT. Patterns of use of dry powder inhalers versus pressurized metered-dose inhalers devices in adult patients with chronic obstructive pulmonary disease or asthma: An observational comparative study. Chron Respir Dis 2017;14:309–320.
- Ibrahim M, Verma R, Garcia-Contreras L. Inhalation drug delivery devices: technology update. Med Devices (Auckl) 2015;8:131–139.
- Price DB, Román-Rodríguez M, McQueen RB, et al. Inhaler errors in the CRITIKAL study: type, frequency, and association with asthma outcomes. J Allergy Clin Immunol Pract 2017;5:1071–1081.
GINA strategy recommendations
- Global Initiative for Asthma (GINA 2021). Global strategy for asthma management and prevention. Last accessed July 2021. Available from: ginasthma.org.
Recent clinical trials
- Global Initiative for Asthma (GINA). 2021 GINA Report, Global Strategy for Asthma Management and Prevention. Volume 2021, 2021.
- Kerstjens HA, Engel M, Dahl R, et al. Tiotropium in asthma poorly controlled with standard combination therapy. N Engl J Med 2012;367(13):1198-1207.
- Lee LA, Bailes Z, Barnes N, et al. Efficacy and safety of once-daily single-inhaler triple therapy (FF/UMEC/VI) versus FF/VI in patients with inadequately controlled asthma (CAPTAIN): a double-blind, randomised, phase 3A trial. Lancet Respir Med 2021;9(1):69-84.
- Virchow JC, Kuna P, Paggiaro P, et al. Single inhaler extrafine triple therapy in uncontrolled asthma (TRIMARAN and TRIGGER): two double-blind, parallel-group, randomised, controlled phase 3 trials. Lancet 2019;394(10210):1737-1749.
- Kerstjens HAM, Maspero J, Chapman KR, et al. Once-daily, single-inhaler mometasone-indacaterol-glycopyrronium versus mometasone-indacaterol or twice-daily fluticasone-salmeterol in patients with inadequately controlled asthma (IRIDIUM): a randomised, double-blind, controlled phase 3 study. Lancet Respir Med 2020;8(10):1000-1012.
- Gessner C, Kornmann O, Maspero J, et al. Fixed-dose combination of indacaterol/glycopyrronium/mometasone furoate once-daily versus salmeterol/fluticasone twice-daily plus tiotropium once-daily in patients with uncontrolled asthma: A randomised, Phase IIIb, non-inferiority study (ARGON). Respir Med 2020;170(106021).
- Hardy J, Baggott C, Fingleton J, et al. Budesonide-formoterol reliever therapy versus maintenance budesonide plus terbutaline reliever therapy in adults with mild to moderate asthma (PRACTICAL): a 52-week, open-label, multicentre, superiority, randomised controlled trial. Lancet 2019;394(10202):919-928.
- Beasley R, Holliday M, Reddel HK, et al. Controlled Trial of Budesonide-Formoterol as Needed for Mild Asthma. N Engl J Med 2019;380(21):2020-2030.
- van Zyl-Smit RN, Krüll M, Gessner C, et al. Once-daily mometasone plus indacaterol versus mometasone or twice-daily fluticasone plus salmeterol in patients with inadequately controlled asthma (PALLADIUM): a randomised, double-blind, triple-dummy, controlled phase 3 study. The Lancet Respiratory Medicine 2020;8(10):987-999.
- Kornmann O, Mucsi J, Kolosa N, et al. Efficacy and safety of inhaled once-daily low-dose indacaterol acetate/mometasone furoate in patients with inadequately controlled asthma: Phase III randomised QUARTZ study findings. Respiratory Medicine 2020;161(105809).
of interest
are looking at
saved
next event
of interest
are looking at
saved
next event

Developed by EPG Health for Medthority in collaboration with Novartis Pharma AG, with content provided by Novartis Pharma AG. The views presented in the videos are those of the presenters and not necessarily those of the industry sponsor, Novartis Pharma AG. Any data on non- Novartis products are based on publicly available information at the time of content update. Prescribing information may vary depending on local health authority approval in each country. Before prescribing any product, always refer to the SmPC or product information approved in your local country. Inhaled management of asthma and recent clinical trials: MLR ID: 137988; FUSE ID: 72716. GINA strategy recommendations: MLR ID: 137985; FUSE ID: 72715. Images are of models, used for illustrative purposes only.